
Why are doctors so unwilling to run tests?
It is impossible to get the average doctor to act like a scientist instead of a bureaucrat.

I.
I’ve been hiccuping for nearly 70 hours. We are well past the stage of ‘huh this is funny’ and well into the stage of ‘what the FUCK is going on?!’ It’s reached the point where, when I call medical professionals, they do what I can only imagine is a spit take. “Wait, you’ve been hiccuping for how long?!” I can’t live like this, I have events I need to go to! I can’t like, show up to a speaker series or a client demo or a candidate interview and just be hiccupping the whole time! The only upshot is that my abs are getting the best workout they have had since I was on the highschool jv waterpolo team (go big blue).
Hiccupping is one of those weird things where we kinda sorta don’t really know what causes them. Like, mechanically, we get it. It’s a spasm of your diaphragm. Why does the spasm happen? Well there are these nerves that exist that get irritated sometimes and mumblemumble and then you have hiccups. And then when you point out the doctor just said ‘mumblemumble’ they get annoyed at you.
Hiccupping is also one of those weird things where we don’t really have any obvious targeted medications for it. I mean, there are approximately a million different home remedies. Swallow some air, sip water slowly, sip water quickly, sip cold water, sip warm water, eat a spoonful of a peanut butter (thanks Raymond!), each a spoonful of crushed ice, eat a spoonful of granulated sugar, hold your breath for 5 seconds, hold your breath for 10 seconds, hold your breath for 20 seconds and then sip some air (temperature unspecified), pull your legs into your chest, do the bridge yoga pose, do jumping jacks, and, of course, drink water upside down.
Perhaps surprisingly, none of these are respected by the medical establishment. If you show up at the doctor’s office hiccupping for 70 hours, they will not have any obvious treatments for you, and they may not have any great pointers for a diagnosis either.
II.
I’m not a doctor, but my Mom always wanted me to be one, so let’s just imagine I was. If I was a doctor, and I had a patient with some weird symptoms that I didn’t really understand, my first reaction would be ‘huh, interesting’ and my second reaction would be ‘we need to collect more data.’ And I would then go and order every test under the sun to try and figure out what was going wrong. Claude says that a really comprehensive blood panel costs somewhere between $25-50 to do — that’s the cost of the reagents and the labor and the blood draw supplies and so on. Let’s throw on a really comprehensive stool test too, which would add another $120-150. So the total is somewhere between $150-200 to get a ton of data about the patient.1 This seems obviously useful.
But I am clearly not a doctor, because no doctor seems to agree with me. Every medical professional that I have ever seen — including the two doctors and two nurses I saw at urgent care, and the doctor and nurse I saw at Mt. Sinai — has basically refused to do this kind of data gathering. Instead, they will take a stab at some cause based entirely on the medical history and a few words with the patient, propose some medication that treats that cause, and then refuse to budge at all from that initial guess.
For my hiccups thing, that initial guess was gerd. All three doctors heard that I had eaten Indian food and went “yup, you have acid reflux.” Nevermind that it has been three days since I last had Indian food, and that in that time I had only eaten bread and rice, and that I had already taken several doses of acid suppressants by the time the third day rolled around, and the fact that I am ethnically Indian and eat Indian food all the time.
The third time a doc told me that a) I had to keep taking the omeprazole and pepsid (acid suppressants) that I was already on and b) they weren’t going to give me anything else, I nearly lost it.2 I had to basically force the doc to put in an order for a blood panel and an H. Pylori test.3 And I forgot to also push for a stool test, which I’m still banging my head over.
When I first mentioned that I should get tested for H. Pylori, the doctor saw that I had taken a single dose of a proton pump inhibitor (PPI) and went “nope, sorry, you can’t take that test until you’ve completed a 4 week PPI course and then waited another 2 weeks for the PPI effects to wear off.” This is because taking a PPI can increase the likelihood of false negatives. I had to patiently explain that even if the medication did increase the false negative likelihood, we would still get a lot of useful information if the test came up positive, and that starting treatment 6 weeks earlier would be incredibly helpful. The doc was clearly unhappy with this line of reasoning, and pushed back at least three times before acquiescing.
I did eventually get the test order in, but then when I went downstairs to labcorp the guy there saw that I was on a PPI, saw that I was trying to get an hpy test, and decided that I wasn’t supposed to take it. He first tried calling the doctor, and then made me go back upstairs to get a signature from the same doctor that I’d already done three rounds with. Which I did. And then while I was waiting, a different doctor from the same practice called the labcorp guy back, both of them agreed that I shouldn’t take the hpy test, and it wasn’t until I got on the phone with the second doctor and explained the whole false positive thing that these people finally agreed to give me this test. Which, by the way, just involves blowing into two balloons and drinking some lemonade.
I got to the doctor’s at 9AM and left at noon. A quarter of my day, gone. I’ll get the results back in a few days, hopefully.
III.
If you read the title, this is obviously not a story about hiccups. This is an article about the ridiculousness of dealing with the US medical system while suffering from some random ailment that no one understands.
I’ve written about my dealings with the US healthcare system before. That post is one of my favorite articles, and my only regret is that I did not write it when I had a bigger audience — I had 54 subscribers when I first posted it. You should go read it:

In that post, I said "healthcare in the US is an exercise in indignities.”
It’s been ~two years since I wrote that post, and nothing has changed.
It’s easy to look at the story above and see a microcosm of everything wrong with how US healthcare works. There’s a fragmented healthcare system where most of the medical professionals did not see relevant medical history information like the previous H. Pylori diagnosis or the fact that I have EOE. There’s the difficulty in getting an appointment — I only ended up being seen by an actual GI because the lady on the phone took pity on me for not being able to get through two words without hiccupping.4 There’s a ridiculously expensive markup on everything. I paid ~$200 to see my providers and get the meds they prescribed, and I’m on pretty good health insurance.5
But in my opinion, the worst thing is that it is impossible to get the average doctor to act like a scientist instead of a bureaucrat.
Bluntly, I have a very hard time rationalizing why a doctor would hesitate to order tests.
IV.
But lets try anyway. A few possibilities, roughly ordered by most to least generous:
The base rate for most diseases is very low, so the actual statistical likelihood of false information from any given test is quite high. Since these tests can lead to unnecessary treatment with real side effects (or at least, anxiety) it’s better to not do ‘data gathering’ tests.
Insurers won’t cover it.
Most patients get ~15 minutes with the doctor, which isn’t enough time to really go through and get a detailed analysis that would lead to a good idea of what tests to prescribe, and it’s much more efficient (and gets more $$$) to simply shoot from the hip.
Doctors don’t want to admit they don’t know something.
In the interest of fairness, I talked to a few friends of mine who worked in healthcare and sent them a draft of this post.
First, my old college friend Omid, who is now a doctor (a statement that I am both incredibly proud of and mildly mildly terrified by).
Off the bat he was pretty surprised by the baclofen diagnosis:
Which, yea, based on my initial experience, that was weird choice to tell me to take that every 8 hours! He recommended gabapentin instead and spent a fair bit of time bashing urgent cares.6 Starting to understand why Mom always wanted a doctor in the family.
Omid pointed out that most doctors in the NYC area in particular are extremely triage focused. EDs just get so much random inflow from people who may have annoying symptoms but are just clearly not in any real medical emergency, coupled with way too many people who are at severe risk of dying right now. If you are not in the latter category, you are essentially told to go home and figure it out. That’s not to say that every doctor’s office is treated like an emergency room. But most doctors do end up doing some ED shifts, especially at the big research hospitals (Sinai, Langone, MSK, Rockefeller…). So the culture leaks through.
He also said that Occam’s razor is a meaningful part of med school training. Basic labs and an xray are cheap and easy to do. But why even bother doing all that? Yea, fine, testing may provide more data, but empirically the first line treatment generally works!7
My friend David, who works in health insurance, basically agreed on the latter point. I’m going to just quote him directly:
[From the insurance side] the tradeoffs here are individual versus macro scale optimization of health outcomes + patient comfort, while optimizing and operating under constrained resources ($, limited numbers of medical machinery, limited numbers of providers, limited numbers of providers with the appropriate specialty).
The idea is that we only dedicate resources at scale to the things with high signal to noise ratio, and the highest signal is patient discomfort.
In your case, that discomfort requirement is clearly met. But that doesn’t mean jumping straight to a test is best for society as a whole -- the symptoms may resolve on their own / with medication before you’d even get the results back, the test may/may not find anything, etc.
“Do the thing cheapest/least resource intensive thing that’s likely to work first, then move on to the alternative.”
He even made this cool graph:
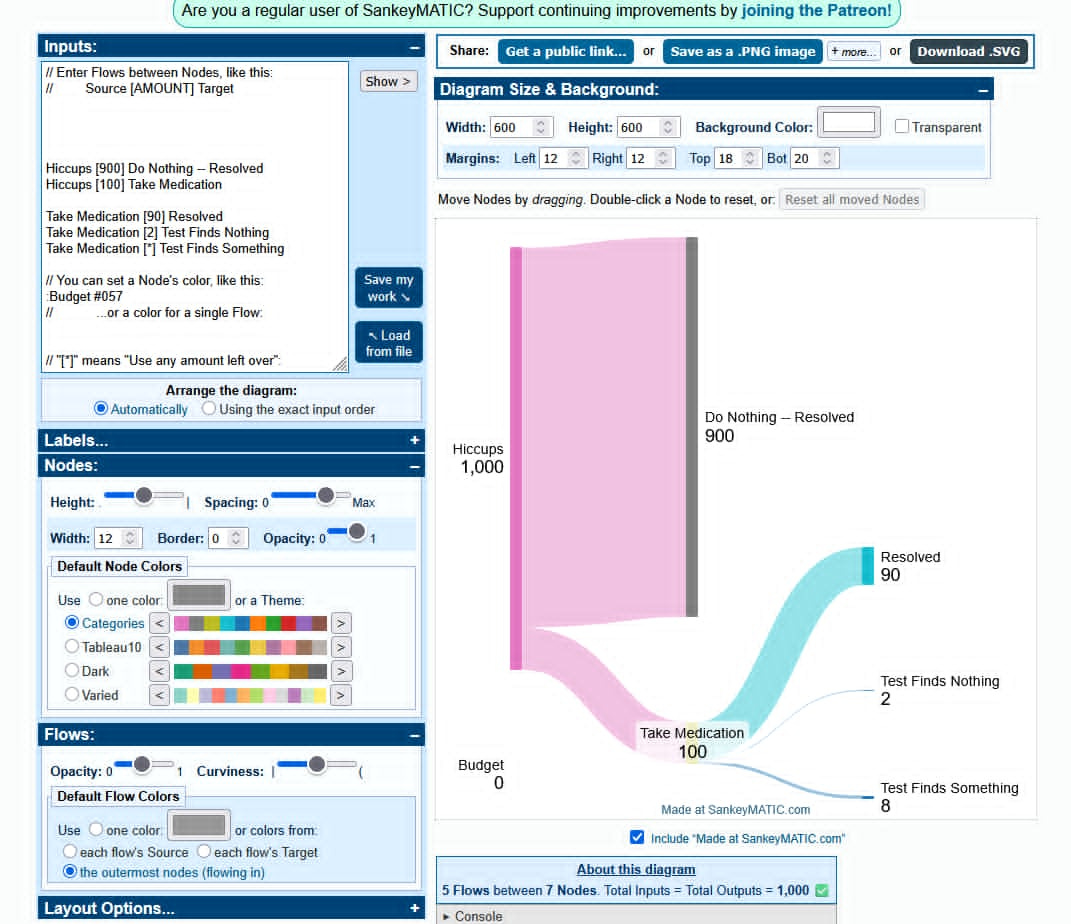
My friends are (generally) reasonable people, and they (generally) say reasonable things, and all of this is, shockingly, pretty reasonable. Like, yea, that makes sense, doctors aren’t twirling mustaches and even if I (a patient) want more love and attention, I (a member of society) recognize that in the grand scheme of things my hiccups are simply not life threatening even if they are supremely annoying.
It would be convenient if there was just a stupid reason for doctors to hate tests, because then I could at least put my incades-hic-ent rage at these hiccups somewhere. But no one sets out to be a villain, and everyone is responding to incentives.
V.
But I still think the incentives of this system are fucking stupid.
At a societal level the goal ought to be quality-adjusted-life-years (QALY), not fastest-and-cheapest-treatment-of-symptoms-that-make-the-patient-go-away.8 And though I am not an expert, I assume that the best way to improve QALY is by getting at the root cause of a thing and actually fixing it. Most of the time, the first-line treatment for a bunch of symptoms works because we have an accurate read of the underlying disease being treated.
I think you could maybe mount an argument that testing actually reduces QALY, because most tests are very likely to false positive (thanks, Bayesian statistics). David had a great line:
If you go looking for an abnormality in a human body, you will always find one.
But even here I am unconvinced.
First, doctors are supposed to be the ones interpreting the information that they get from tests.9 I think it is probably true that the average lay person won’t understand what a false negative is or why a PPI may result in one for an H. Pylori test. But why does that even matter? The lay person shouldn’t be responsible for interpreting anything. The doctor should just prescribe the test and then interpret the data the way they were trained to.
Second, this clearly doesn’t apply in a situation where the first guess is obviously wrong and waiting for six weeks won’t do anything. When all bets are off, why are we still mechanically clinging to the script?
And third, there obviously are doctors who are totally willing to get in the weeds with a patient and order a battery of tests and figure out what is actually going on. These are some of the best doctors in the world!
I think the real kicker, the thing that really ticks me off, is that tests are by all accounts cheap to produce and cheap to administer. Far cheaper than prescribing the wrong thing and wasting the patient’s and the doctor’s time with a follow up. Every trip to the ER almost always results in a suite of tests, as does every physical. Hell, they’ll take your blood pressure and temp and oxygen levels before you even see a doctor. They’re thrilled, they’re practically jumping for joy to take your blood pressure / temp / O2. I don’t think these tests are all that different from a blood panel or a stool test. And I just refuse to believe that we’ve coincidentally settled on the exact optimal amount of testing for every person, which just so happens to be ‘once a year-ish.’
The growing ‘preventative optimization’ and ‘longevity’ industries seem to agree with me — these are all about extremely comprehensive full body testing, catered to folks who are willing and able to pay. Because these medical practices prescribe tests more often, they are able to evaluate deltas off the patient’s baseline instead of what we do today where we try to fit everyone into the same standard box. I know that the jury is still out on the efficacy of these things, I know that the longitudinal studies have not yet come back. But also, I have way too many friends with some story like “I was lethargic and sick all the time and then I took one of these tests and discovered I have celiac, and now I just avoid bread and I feel better than ever” (and then they proceed to do a triple backflip or whatever). Whatever amount of money we are spending on making tests cheaper and more accessible is simply not enough.10
At the end of the day I am an empiricist and a scientist. Data is in my blood.11 I know there are a lot of big systemic problems with healthcare in the US. But this tiny thing just frustrates me to no end. Make it ok to order tests for patients.
(Also, if you have any remedies for long lasting hiccups, ideally ones that do not prevent me from operating heavy machinery, let me know)
Note that the price that is actually charged is, of course, totally disconnected from the price of materials, and is something like 10x this number. But that’s a different problem for a different article.
I want to note that the second doctor I saw did prescribe baclofen, a muscle relaxant. He was also pretty skeptical that it was gerd, but also didn’t want to order more tests. He basically was like, take the baclofen every 8 hours for a week, it may break the cycle, and you should see a GI for more tests. Baclofen is pretty fucking strong! A single dose knocked me out so hard I went to sleep at 7pm and woke up at 8am the next day (13 hours of sleep, after which I woke up hiccuping). What do you mean ‘take it for a week and wait and see’?! I have a life to live!
H. Pylori is a fascinating little devil, by the way. It’s an infection of the stomach. You know, that thing that is normally filled with acid so strong that children’s TV shows always have an episode of someone nearly dying in the stuff? The folks who discovered H. Pylori got a Nobel Prize in Medicine because the entire rest of the world assumed the stomach was naturally sterile. Let me tell you, H. Pylori is designed to survive, and it is near impossible to kick. They put me on some obscene antibiotics to finally get rid of it. I’m not talking about amoxicillin, that’s some baby shit. Talk to me when you’re on metronidazole and enough pepto bismol to turn your stool black. Did I mention that most H. Pylori strains have antibiotic resistance?
My usual GI didn’t have an appoint available until June. For all the people who talk a big game about how Canada and the UK have big lines to see doctors, guess what! We have big lines too!
I am uncertain, but I suspect insurers were billed at a 10x mark up.
“Urgent care is not real medicine tho, it’s just for flu and STIs lol.”
I did not contest him on the empirics. Claude points out that it really depends on what exactly is being treated — things like bacterial infections have an above 80% response rate to first line treatment, and also are way more common than, like, treatment-resistant depression or H. Pylori. And none of this really gets at the thing that I’m actually interested in, which is “how often is the doctor’s diagnosis correct?” and which is way more difficult to actually measure.
The latter does not have a convenient shorthand.
Though this is maybe not as much a slam dunk as I want it to be, since studies have repeatedly shown doctors don’t understand Bayesian statistics.
Especially in a world where we have magic thinking machines that excel at crunching and finding patterns in reams and reams of data!
Double meaning intended.
Pro tip for dealing with doctors, kids! If the doctor says "No" to a test, then say these magic words: "I would like you to make a note in my chart that I specifically requested these tests, and that you refused".
It's *AMAZING* how often they'll change their minds, if you ask them to document their logic!
The flip side of that is that if they *do* refuse, you should take it as STRONG Bayesian evidence that their perspective is correct, and should spend a lot of time doing research on the issue before you pull that again; you should also probably be prepared to eat some humble pie on your next doctor visit, when you recap what you've learned, and why you now agree with the doctor. Not guaranteed of course, just a likely outcome.
In short - yeah nobody knows but the vagus nerve is part of the reflex pathway. Two ways to reset it:
1. Try the hiccaway straw if you haven't yet.
2. Stick your face in a bowl of ice water.